プラットフォーム
内視鏡・病理・放射線を横断する、一つのAIネイティブなプラットフォーム。
エッジとポッドの2層からなるAIネイティブPACS — オンプレミスまたはハイブリッドで、DICOMとHL7上に、既存のシステムに適合して導入します。
2つのレイヤーで構成されるAIネイティブなPACS: edgeとpod
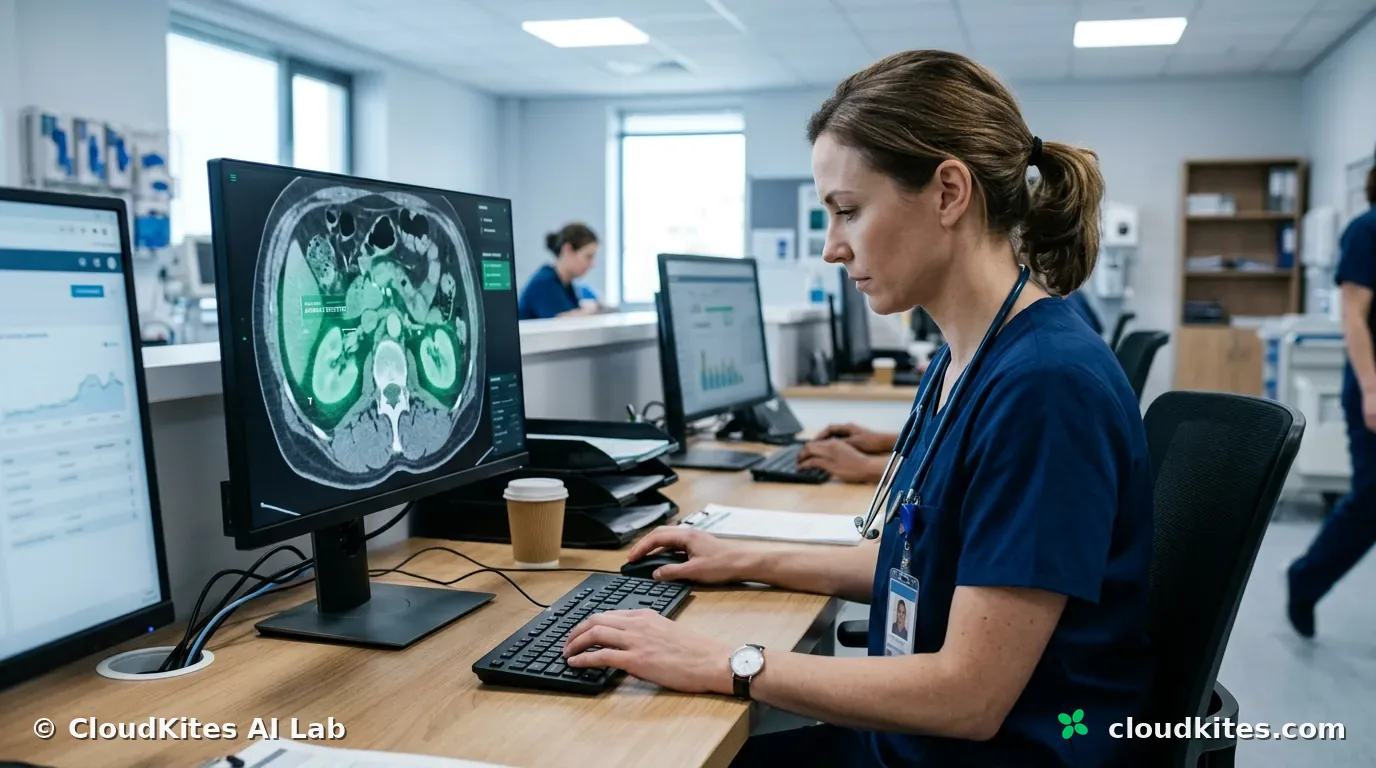
CloudKitesは2つのレイヤーで構築されたAIネイティブなPACSです。edgeソフトウェア — EndoEdge、PathoEdge、TomoEdge — は診療現場で医療従事者をリアルタイムに支援します。その背後にあるpod — EndoPod、PathoPod、TomoPod — は情報システムであり、アーカイブでもあり、選択に応じてオンプレミスまたはハイブリッドで展開でき、段階的に組み込まれるモデルでAI支援に対応できます。
- EndoEdge + EndoPod — リアルタイム内視鏡AIと完全な内視鏡情報システム。
- PathoEdge + PathoPod — ホールスライドイメージング、検査室情報システム、病理AI。
- TomoEdge + TomoPod — 放射線科のためのAIネイティブなRISとPACS。

プラットフォームがどう連携するか
各モダリティには診療現場のedgeツールと、情報システム兼アーカイブとしてのpodがあります。edgeは支援し取り込み、podは整理し同期し下書きを作成します — 臨床医が全工程を通じて確認・編集・署名します。
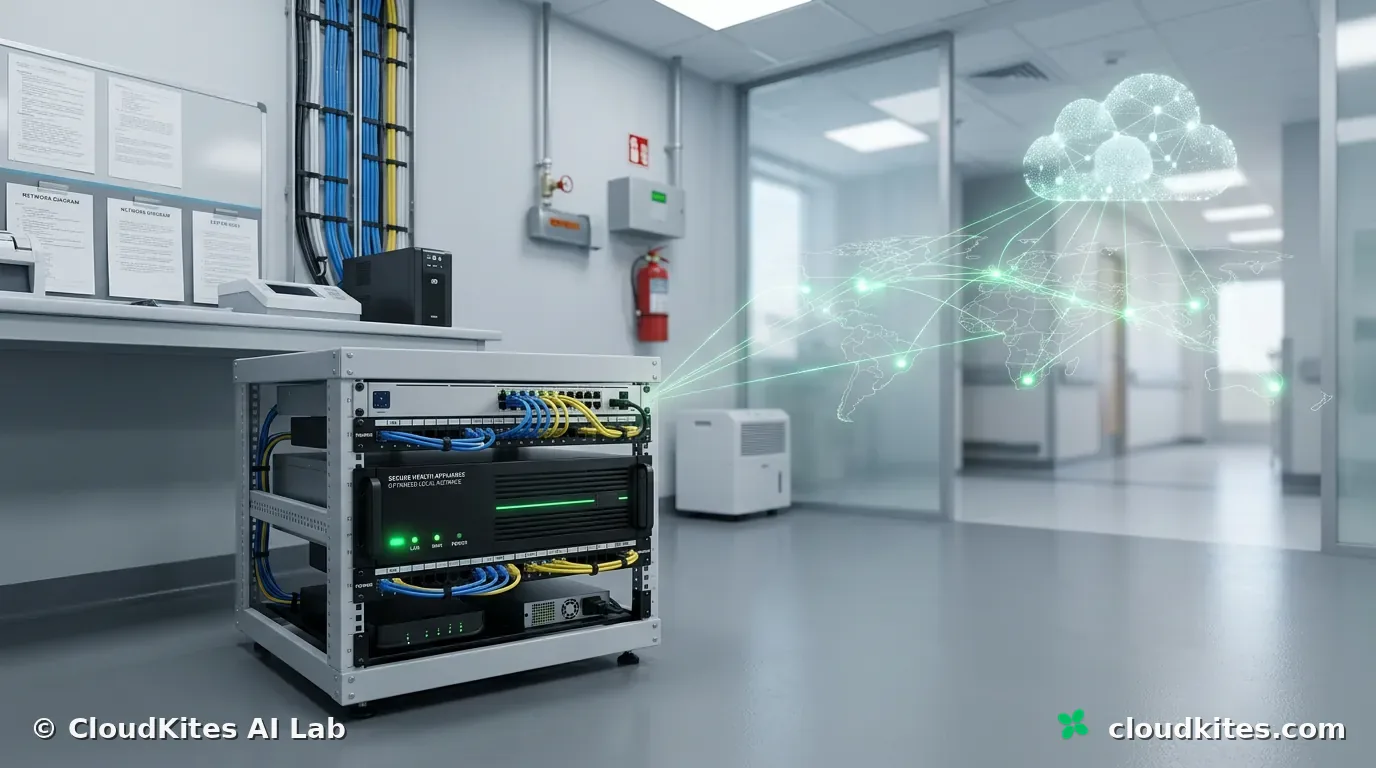
オンプレミスまたはハイブリッド
podがどこに置かれるかはあなたが選びます
podは情報システムでありアーカイブでもあります。そしてどこで稼働するかは、プラットフォームが代わりに決めるのではなく、お客様が下す決定です。
ある部門はすべてを自分たちの壁の中にとどめたいと望み、別の部門はレビューや教育、あるいは第二の拠点のためにクラウドの広がりを求めます。CloudKitesは勝者を選びません。podは完全にオンプレミスで稼働し、アーカイブと情報システムを施設内に保つことができます。あるいはハイブリッドで稼働させることもできます — オンプレミスのpodをクラウドのpodと組み合わせ — 両者は非同期で同期を保つため、edgeは中断中も動き続け、検査はそれを必要とするあらゆる場所で参照可能になります。構成はあなたのものであり、あなたが変わるのに合わせて変えられます。
同じ柔軟性は逆方向にも働きます — 規模の面で。アーキテクチャは小さな単一クリニックから中〜大規模の病院まで、動作を変えずに柔軟に対応します。小規模な解剖病理ラボはPathoPodをLISとして運用でき、多忙な放射線科は完全なAIネイティブのRISおよびPACSとしてTomoPodを運用でき、内視鏡部門はEndoPodをEISとして運用できます。成長に合わせて容量とモダリティを追加していけば、初日に知っていたプラットフォームがそのまま使い続けるプラットフォームになります。
ひとつの基盤
3組のedgeとpodのペア、ひとつの基盤
内視鏡、病理、放射線は3つの異なる世界のように見えます。その下では、それぞれがひとつのAIネイティブな基盤上のedgeツールとpodです — そしてそれは、使う人々にとって実際の結果をもたらす選択です。
それぞれが独自の習慣、独自の癖、何が安全かについての独自の定義を持つ3つの別々の製品を作るほうが簡単だったでしょう。多くのソフトウェアはそのように、一度に1チームずつ成長し、やがて継ぎ目が見えてきます。CloudKitesはあえて難しい道を選びました。ひとつのAIネイティブな基盤を、各モダリティ向けのedgeツールとpodとして表現するという道です。内視鏡医、病理医、放射線科医は、それぞれの専門に合わせて形づくられたツール — EndoEdgeとEndoPod、PathoEdgeとPathoPod、TomoEdgeとTomoPod — を目にしますが、彼らは同じ地面の上に立っています。
その成果は、モデルが断片化しないことです。edgeはリアルタイムに支援し取り込み、podは情報システム — EIS、LISまたはRIS — として、検査をDICOMでカプセル化し、HIPAAを意識した姿勢でHL7に整合します。展開は選択に応じてオンプレミスまたはハイブリッドです。AIは段階的に組み込まれ、顧客ごとにカスタマイズできます。そして臨床医は半自動の報告書を確認・署名し、意思決定の輪の中にとどまります。部門が2つ目や3つ目のモダリティを追加するとき、2つ目や3つ目の働き方を学ぶわけではありません。すでにこの方法を知っているのです。
より静かな利点もあります。共有された基盤は、あるモダリティで役立つモデルを次のモダリティへ拡張でき、ある場所で満たされた標準がどこでも満たされた標準になることを意味します。プラットフォームは切り離された断片としてではなく、全体として良くなっていきます — そして、こうしたことを考えたいなどと一度も望まなかった臨床医は、edgeツールが支援し、podがどこで出会っても同じように振る舞うことに気づくだけです。
製品
同じ標準で構築された3組のedgeとpodのペア。
共有モデル
すべての製品で変わらず保たれること
下の表は要約です。各行の背後には、あるモダリティから次のモダリティへと移っても曲がらない原則があります。
2層構造はその第一です。すべての製品は診療現場のedgeツールに、情報システムでありアーカイブでもあるpodを加えたものです — そしてそのpodは顧客の選択に応じてオンプレミスまたはハイブリッドで展開でき、決して押し付けられることはありません。第二は、すべてが標準に基づいていることです。検査はDICOMでカプセル化され、システムはHL7およびHIPAAに準拠するよう構築されているため、podは病院環境から切り離されるのではなく、その中に収まります。これらのいずれも製品ごとの決定ではなく、両方とも構造上どこでも成り立ちます。
第三はAIの姿勢です。特定のタスクのために段階的に組み込まれ、顧客ごとにカスタマイズでき、臨床医が常に確認・編集・署名する半自動の報告書を作成する、プラグイン可能で拡張可能なモデルです。プラットフォームのどこにも自律診断はありません — 何かが記録に達する地点では人間が意思決定の輪の中にとどまります。これら3つが揃ったものはマーケティングのリストではありません。それはプラットフォームが、それに頼る人々と結ぶ契約であり、その契約は作業が内視鏡であれ病理であれ放射線であれ同一です。
すべての製品で共有
| EndoPod | PathoPod | TomoPod | |
|---|---|---|---|
| 診療現場でのリアルタイム支援 | ✓ | ✓ | ✓ |
| 情報システム (EIS / LIS / RIS) | ✓ | ✓ | ✓ |
| Webベースのビューアー | ✓ | ✓ | ✓ |
| オンプレミスまたはハイブリッド展開 | ✓ | ✓ | ✓ |
| DICOM、HL7、HIPAAに配慮 | ✓ | ✓ | ✓ |
| プラグイン可能なAI、半自動の報告書 | ✓ | ✓ | ✓ |
| 臨床医が確認・署名 | ✓ | ✓ | ✓ |